
Endogenous vs. Exogenous Insulin
Endogenous Insulin:
Insulin is a peptide hormone produced by β-cells of the pancreatic islets of Langerhans that comprise the endocrine pancreas.

C-peptide has a longer half-life than the mature insulin cleavage product. The detection of this C-peptide (especially in the fasting state) is a useful indicator of the insulin secretory capacity of the β-cells.
Thus, C-peptide is useful for determining if a patient has insulin deficiency (as with diabetes) or insulin excess (as with hyperinsulinism leading to recurrent hypoglycemia).
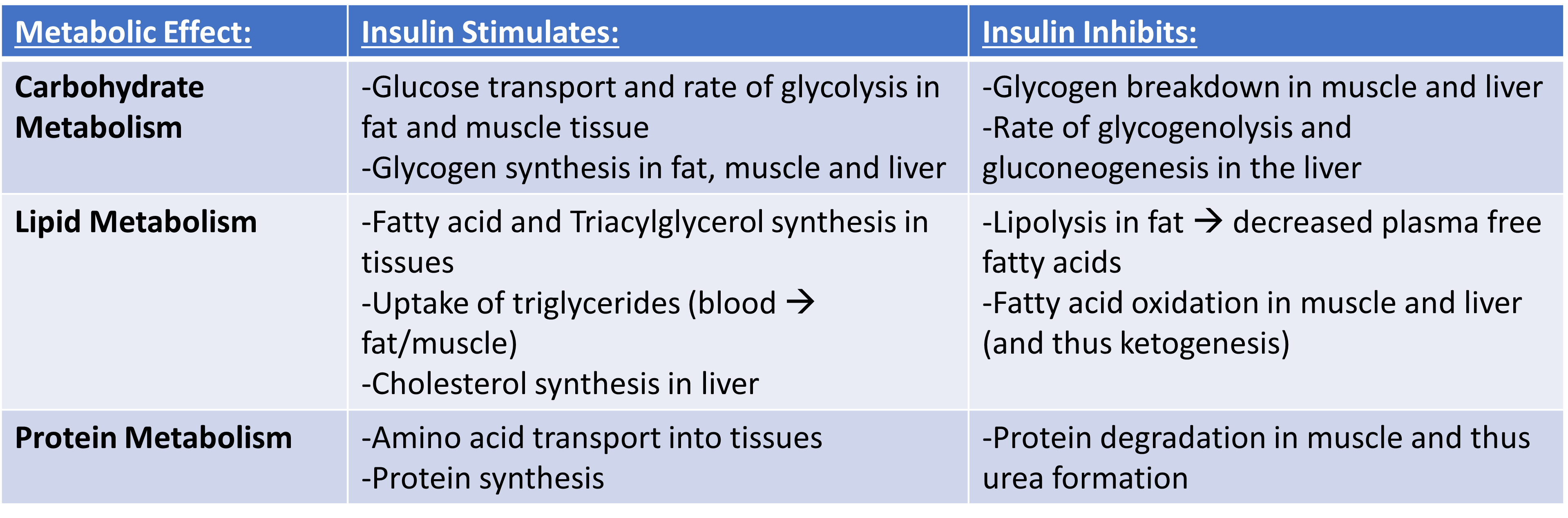
Insulin acts upon insulin receptors in various target organs leading to its overall anabolic effects related to carbohydrate, lipid, and protein metabolism as summarized in Table 1.
Exogenous insulin used in insulin-replacement therapy is synthetic insulin that is mass-produced using recombinant DNA technology and is based upon the amino acid sequence of mature human insulin.
As C-peptide is not produced in the manufacturing process of insulin analogs, a patient with recurrent hypoglycemia with detectable insulin levels and absent C-peptide should raise suspicion of surreptitious self-insulin administration in children without diabetes.
Quiz Yourself:
Bibliography:
- Chapter 7. Endocrine pancreas. Molina P.E.(Ed.), (2013). Endocrine Physiology, 4e. McGraw Hill. https://accessmedicine.mhmedical.com/Content.aspx?bookid=507§ionid=42540507

Feedback/Errata