
9 Hypopharynx
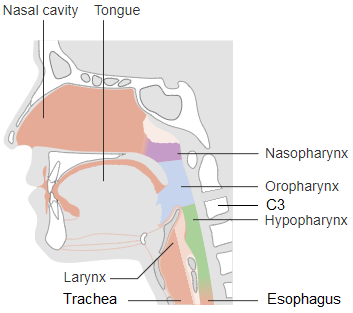
The hypopharynx, also known as the laryngopharynx, extends from the hyoid bone to the esophagus. The epiglottis is the superior border, at the level of C3. The hypopharynx is posterior to the larynx and is comprised of the “3 P’s” – the pyriform sinuses, posterior cricoid, and lower posterior pharyngeal walls. The pyriform sinuses are the most common location for cancer within the hypopharynx. It commonly spreads to lymph nodes and invades nerves and muscles nearby. Regarding lymphatics, the hypopharynx drains to the mid-cervical nodes, superior deep, middle, and low jugular nodes, and retropharyngeal node (Node of Rouviere). Due to the rich lymphatic supply of the area, approximately half of all patients will be diagnosed with positive lymph nodes.
Patient Simulation: Hypopharynx
The simulation process is consistent with the typical head and neck in treating hypopharynx lesions. Please refer to the “Patient Simulation: H&N” section.
Treatment Volume Localization: Hypopharynx
Traditional treatment borders for the hypopharynx are:
- Superior: inferior aspect of the mandible and mastoid process to the base of the skull
- Anterior: in front of thyroid cartilage with a margin around tumor extension
- Posterior: behind spinous processes with a margin on all nodal disease
- Inferior: below the cricoid cartilage, to encompass the entire extent of the tumor with a 1.5-2cm margin or to include the lower jugular and supraclavicular area.
Treatments today still follow these general borders but are more conformal to targeted tissues, sparing normal tissues and reducing toxicity. Please refer to the “Treatment Volume Location: H&N” section.
Treatment Techniques: Hypopharynx
Historically, opposed lateral fields treat to 45 Gy, and beam size is reduced off the spinal cord to deliver 65 Gy to the primary tumor volume. Preoperatively, 45-50 Gy is given, followed by a laryngopharyngectomy. Postoperatively, 50 Gy is delivered in 6 weeks via lateral fields. An additional 10-20 Gy may be delivered to the stoma if the surgical margins are not clear of disease. Modern treatment techniques are consistent with the typical head and neck protocol in treating the hypopharynx and are reflected in the “Treatment Techniques: H&N” section.
Media Attributions
- Picture16 adapted by Jared Stiles is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}