
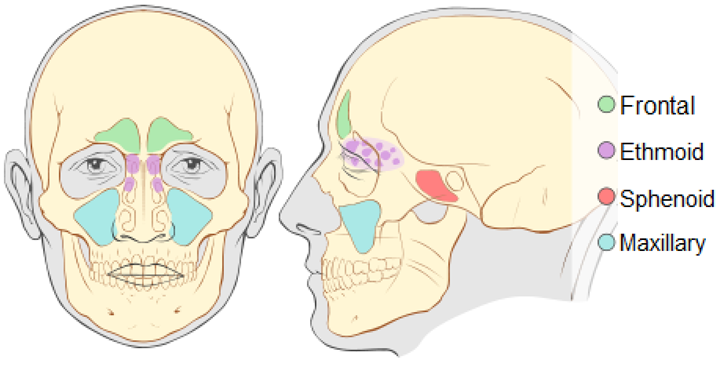
12 Sinuses
The maxillary sinus is the largest sinus and the most frequently involved site of malignancy. 80% of maxillary sinus tumors are squamous cell carcinoma, and about 15% are adenocarcinomas. Primary tumors of the frontal sinuses or sphenoid sinuses are exceedingly rare; they comprise about 5% of head and neck cancers in the United States.
Simulation Overview & Special Considerations: Sinuses
In treating sinus cancers, the simulation process is consistent with the typical head and neck simulation. Please refer to the “Patient Simulation: H&N” section. Depending upon the disease location, patients may benefit from the use of a bite plate or tongue depressor to reduce dose to the oral tongue.
Treatment Volume Localization: Sinuses
Historically, maxillary antrum tumors were treated with conformal anterior and lateral wedged fields. A contralateral field is sometimes necessary to improve the uniformity of the dose distribution. The lateral field must enter posterior to the eye on the involved side and be angled posteriorly away from the contralateral eye. IMRT provides a more conformal dose distribution to the unusual PTVs in sino-nasal cancer, which are used today. Treatment borders depend upon tumor location and extent of the disease, but general borders for the all sinuses include:
Anterior field borders:
- Superior: 2 cm above the cribriform plate – It is important to have the patient look straight ahead to avoid over-dosage to the retina.
- Inferior: lateral commissure of the lip (this will provide a margin on the lower border of the maxillary sinus) to include the alveolar ridge.
- Medial: 1.5-2cm across the midline to include the ethmoid sinus and the medial aspect of the contralateral orbit.
- Lateral: to include the entire maxillary sinus tumor extent with an adequate margin (if the infratemporal fossa is involved, fall off is needed laterally).
Lateral field borders:
- Anterior: behind the contralateral bony canthus (the lateral portals can be angled 5 degrees posteriorly to shield the contralateral lens)
- Superior: 2 cm above the cribriform plate and follow the floor of the skull with a margin on the clivus.
- Posterior: includes the pterygopalatine fossa and the nasopharynx with a margin on the posterior extent of the tumor. In patients with nasal cavity/nasopharynx involvement, include the retropharyngeal nodes.
- Inferior: lateral commissure of the lip.
Treatments today still follow these general borders but are more conformal to targeted tissues, sparing normal tissues, and reducing toxicity. Please refer to the “Treatment Volume Location: H&N” section.
Treatment Techniques: Sinuses
Many different treatment techniques can be used for the paranasal sinuses. Initially, surgical resection is recommended if possible. Patients who present with invasion through the posterior wall of the maxillary sinus (invasion of the nasopharynx or base of the skull) are generally inoperable and must be treated with radiation therapy alone. Modern treatment techniques are reflected in the “Treatment Techniques: H&N” section.
The dose-fractionation schemes for sinus cancers include:
- 60 Gy in 30 daily fractions given for 6 weeks OR
- 70 Gy in 35 daily fractions, if possible, where there is residual disease
Palliative dose-fractionation schemes:
- 36 Gy in 6 fractions of 6 Gy, treating once weekly
Media Attributions
- Picture23 adapted by Jared Stiles is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}