
6 Nasopharynx
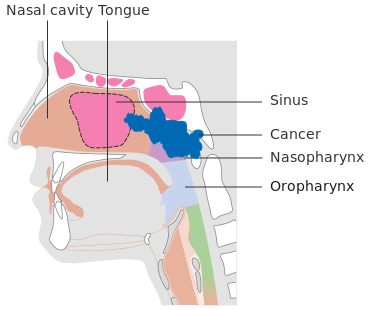
The nasopharynx is a mucosa-lined box-like chamber that is 2 cm wide by 4 cm long. It is posterior to the nasal cavity and bordered inferiorly by the soft palate and oropharynx. Surgical resection in this area is impossible due to the base of the skull. The nasopharynx is a challenging area to examine, making it difficult to detect these cancers early. Tumors of the nasopharynx commonly arise in the roof or lateral wall behind the eustachian tube or orifice and spread via mucosa or submucosa to invade the nasal cavity or the oropharynx. Nasopharyngeal cancer is rare in the United States, but it does occur more frequently in other parts of the world, especially in Southeast Asia.
Patient Simulation Overview: Nasopharynx
The simulation process is consistent with the typical head and neck simulation in treating nasopharynx tumors. Please refer to the “Patient Simulation: H&N” section.
Special Simulation Considerations: Nasopharynx
For patients who are at a higher risk for weight loss, a prophylactic percutaneous gastrostomy tube (PEG) may need to be placed before the patient’s radiation therapy treatments. If possible, one parotid gland should be spared to preserve salivary function. Additionally, bite plates may be beneficial for moving the patient’s tongue down and out of the radiation treatment field.
Treatment Volume Localization: Nasopharynx
Treatment of the nasopharynx is challenging. These cancers typically spreads via direct extension into the soft palate, the nasal cavity, and through the base of the skull. Radiation Therapy is delivered to the primary tumor and local and regional lymph nodes of the neck – even those not directly involved. Regarding lymphatic drainage, the nasopharynx has a rich lymphatic supply, with 80-90% of nasopharyngeal tumors presenting with positive cervical lymph node involvement. Half of these patients will have bilateral lymph node involvement. Therefore, the supraclavicular and the lower cervical lymph nodes are commonly treated due to the high probability of spread.
Common lymph nodes include:
- Retropharyngeal Lymph Nodes: Located anterior to C1 and C2, and they contain the Node of Rouviere.
- Deep Cervical Lymph Nodes: These nodes lie behind the sternocleidomastoid muscle at the junction of the spinal accessory and jugular nodes.
- Jugulodigastric Lymph Nodes
Learn more about lymph nodes of the head and neck.
Treatment Borders for T1, T2 & T3 Nasopharyngeal Tumors:
-
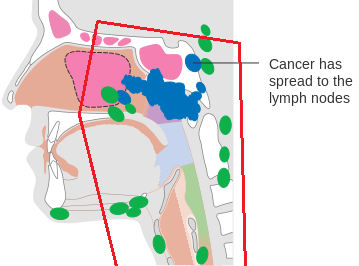
The red lines demonstrate the general field borders for treatments of the nasopharynx. The green circles represent lymph nodes. Anterior: Posterior 2 cm of the nasal cavity, posterior 1/3rd of the maxillary sinus, the posterior ethmoid sinuses, and the posterior ¼ of the orbit.
- Posterior: Behind the spinous processes, including the posterior pharyngeal wall, the deep cervical, the posterior cervical, and the retropharyngeal lymph nodes.
- Superior: The entire sphenoid sinus, the cavernous sinus, and the base of the skull with at least a 0.5 cm margin.
- Inferior: To include include supraclavicular lymph nodes.
For T4 tumors, treatment margins should include the pituitary gland and encompass all intracranial extension.
Treatments today still follow these general borders but are more conformal to targeted tissues, sparing normal tissues, and reducing toxicity. Please refer to the “Treatment Volume Location: H&N” section.
Treatment Techniques: Nasopharynx
Historically, the nasopharynx was treated with opposed laterals and/or anterior oblique wedged fields that are equally weighted. Once the spinal cord reaches the tolerance dose of 45 Gy, an off-cord boost of 15 Gy is delivered; these fields must include the Node of Rouviere because it is a common route of spread. The lower neck and bilateral supraclavicular nodes are treated to 50 Gy in 5 weeks with an anterior yoke field.
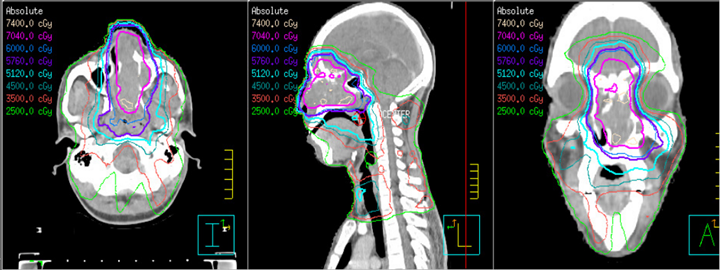
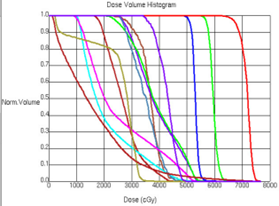
IMRT and VMAT treatments are most often used to treat nasopharyngeal cancers because of the higher dose we can give to the tumor while reducing side effects. Modern treatment techniques are reflected in the “Treatment Techniques: H&N” section.
Common dose-fractionation schemes:
- 70 Gy in 35 fractions over 7 weeks to PTV70 with concomitant Cisplatin.
- Hypofractionation: 74.4 Gy in 120 cGy BID fractions is common.
Media Attributions
- Picture5 is licensed under a CC BY-SA (Attribution ShareAlike) license
- Picture7 adapted by Jared Stiles is licensed under a CC BY-SA (Attribution ShareAlike) license
- Picture9 © The University of Iowa Radiation Therapy Program
- Picture10 © The University of Iowa Radiation Therapy Program
- Picture11 © The University of Iowa Radiation Therapy Program
Lymph nodes in proximity to the primary tumor
The anterior lower neck field of the 3-field technique called "yoke" because its field shape looks like the yoke on a pair of oxen
fewer fractions at a higher dose

{kind=link}
{kind=link}