
19 Pancreas
Overview: Pancreas
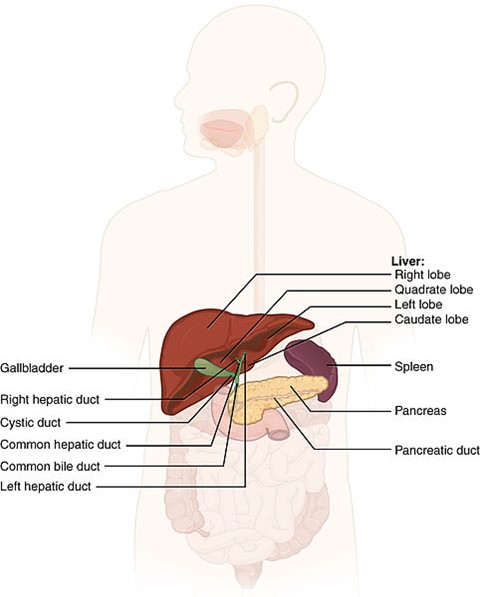
Located at the T12 to L2 vertebral bodies, the pancreas lies retroperitoneally in the upper portion of the abdomen. It is a fish-shaped organ divided into three sections: head, body, and tail. The pancreas is in direct contact with the duodenum, jejunum, stomach, major vessels (IVC), spleen, and kidney. The tail of the pancreas, near the spleen, is the most superior portion, while the head is the most inferior portion and is located in the C-loop of the duodenum. The main lymph node groups of the pancreas include the superior and inferior pancreaticoduodenal, porta hepatis, suprapancreatic, and paraaortic nodes. Due to the abundance of regional lymphatics, most patients have advanced local or metastatic disease at the time of diagnosis. Adenocarcinoma is the most common cell-type but all histology’s carry a very poor prognosis.
Patient simulation & Special Considerations: Pancreas
The simulation process is consistent with the typical abdomen in treating pancreatic cancer. Please refer to Patient Simulation: Abdomen section. The pancreas is highly moveable and can shift locations depending on the fullness or emptiness of surrounding structures. The physician may request patients may be NPO 2-3 hours before treatment.
Treatment Volume Localization: Pancreas
Lymph nodes associated with pancreatic cancer include the pancreaticoduodenal, porta hepatis, suprapancreatic, and celiac nodes. When treating the head of the pancreas, the nodal areas above, and the entire duodenum, must be treated. When the tumor is in the tail or body of the pancreas, the splenic hilar lymph nodes and paraaortic lymph nodes are at risk.
Historically, a 4-field box was used (opposed anterior and posterior fields and opposed lateral fields) to treat pancreatic cancer. The problem with this field arrangement is that the dose delivered to the spinal cord, right kidney, and liver section are higher. Wedges and beam weights are also necessary for treatment planning. Treatment borders for pancreatic irradiation are as follows:
- Superior: the mid or upper portion of T11
- Inferior: include the L3 vertebral body
- Lateral: at least 2/3rds of the right kidney needs to be excluded with a 2-3 cm margin around the tumor or tumor bed
- It is not necessary to include the entire duodenal loop
- The treatment field is extended to the left of the pancreas so that a 3 cm margin around the tumor is created to treat the splenic hilum
- Posterior: vertebral bodies should be split with a one to 2 cm margin beyond the tumor or tumor bed anteriorly
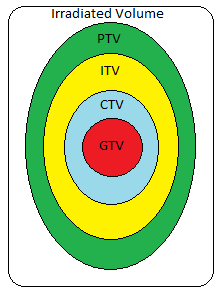
Treatments today still follow these general borders but are more conformal to targeted tissues, sparing normal tissues and reducing toxicity. Because of the difficulty in determining tumor margins, radiologists and radiation oncologists should consult closely to delineate from scans the GTV, including any enlarged regional lymph nodes of 1.5 cm or greater. The CTV should include the visible tumor and the surrounding edema. This area is of considerable uncertainty, and margins must be individually designed. PTV margins are anisotropic with 5-10 mm in the AP direction, 2-4 mm in the transverse plane, and 15-30 mm craniocaudal for organ movement with respiration or abdominal motion and set-up variations. If breath hold techniques or gating is used (ITV), craniocaudal margins may be reduced.
Treatment Techniques: Pancreas
Traditional fractionation for pancreatic cancers is 200-220 cGy with 25-28 fractions. Resectable tumors are usually treated with 45 Gy to the tumor bed, surgical anastomosis, and regional lymph nodes. If critical structure tolerances are not exceeded, a boost to 50-65 Gy may be delivered. Nonresectable cases have a target dose of 50-60 Gy. The typical energy that provides adequate skin sparing on the lateral aspects of the patient while still evenly distributing the requested dose to the tumor is 10 MV photons. The selected energy will depend on the patient’s thickness.
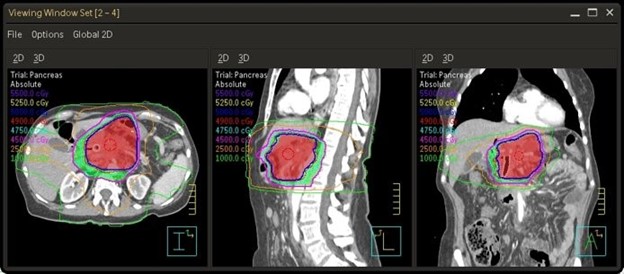
Modern treatments primarily use IMRT and VMAT techniques to treat pancreatic cancer due to their ability to conform to the pancreas and spare surrounding healthy tissue. Common VMAT treatments for the pancreas will consist of two to three complete 360-degree arcs. Studies have shown that IMRT and VMAT treatment techniques further reduce the liver, kidneys, stomach, and small bowel dose compared to 3D conformal treatment. SBRT pancreas fractionation consists of a total dose of 40 Gy delivered in 5 fractions with 8 Gy per fraction. This technique utilizes a treatment every other day; there should be 40 hours minimum between treatments.

Emerging Technologies & Treatments: Pancreas
A pancreaticoduodenectomy, also called the Whipple procedure, is a potentially curative surgical procedure consisting of the resection of the head of the pancreas, entire duodenum, distal stomach, gallbladder, and common bile duct. Reconstruction is done to maintain the continuity of the biliary GI system. The remaining pancreas, bile ducts, and stomach are anastomosed onto various sites of the jejunum. This highly invasive procedure requires lots of recovery time, making it one of the most challenging surgeries for patients but it does offer the best chance of cure. Newer surgical techniques allow this surgery to be complete laparoscopically.
The TIGER-PaC Clinical Trial uses RenovoRX’s innovative therapy platform to evaluate RenovoGem. This clinical trial treats locally advanced pancreatic cancer through intra-arterial delivery of gemcitabine, a systemic chemotherapy agent often used to treat pancreatic cancer. Systemic chemotherapy associated with debilitating side effects may be ineffective in treating pancreatic cancer due to pancreatic tumors lacking blood vessels. The chemotherapy for the TIGER-PaC trial is delivered via an incision in the leg to give the chemotherapy to the targeted tissue across the vessel wall. The primary goal of this clinical trial is to improve overall survival and quality of life for patients with pancreatic cancer.
Proton Therapy: Can help reduce dose to surrounding organs at risk through a reduction in entrance and exit dose. However, organ motion may present a challenge for proton therapy.
Magnetic Resonance-guided Radiation Therapy (MRgRT): Due to abdominal organs’ movability and placement, a popular emerging treatment option is to treat these patients with MRgRT. The radiation delivery via a magnetic resonance linear accelerator (MR-Linac) uses magnetic resonance imaging with radiation to treat cancer patients. A significant benefit of this treatment technique is the ability to provide motion management and real-time imaging during treatment to ensure the target remains in the treatment field and sparing healthy tissue. It also allows the treatment to “Adapt to Shape” or “Adapt to Position” of the malignancy before each fraction. This is ideal for pancreatic cancers because it may be in a slightly different position each day.
Media Attributions
- Pancreas and surrounding anatomy © OpenStax College is licensed under a CC BY (Attribution) license
- Treatment plan for a VMAT of the pancreas © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- Planning target volumes © Jared Stiles is licensed under a CC BY (Attribution) license
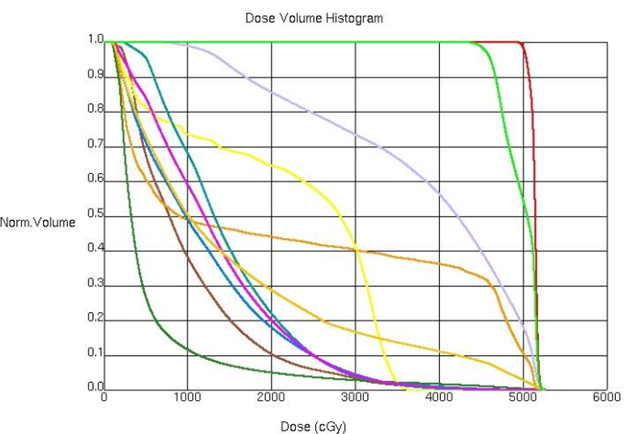
- DVH for a VMAT of the pancreas © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- DVH structures for a VMAT of the pancreas © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
the surgical connection of two channel-like structures

{kind=link}