
24 Rectum & Anus
The rectum is 12-15 cm in length and located between the sigmoid colon proximally and the anus distally. The rectum is divided into three sections: the upper, middle, and lower. The upper rectum tissues drain to the inferior mesenteric, sigmoidal, and sacral lymph nodes. The middle and lower rectum tissues drain to the internal iliac, external iliac, common iliac, presacral, obturator, and inguinal lymph nodes. The sigmoid colon meets the rectum at approximately the third sacral vertebra. The rectum follows the sacral curvature posteriorly. In females, it is attached anteriorly to the vagina; in males, it is bound to the trigone of the bladder, seminal vesicles, and prostate. Due to its location, rectal cancers can invade these adjacent structures.
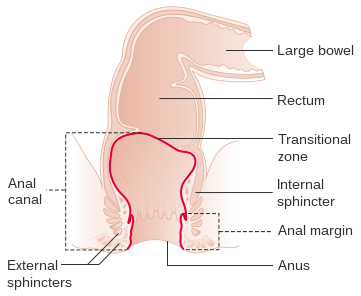
The anal canal extends about 3 cm from the anorectal ring superiorly to the anal verge inferiorly. Rectal and anal cancers commonly spread through direct extension to nearby structures. Transperitoneal implantation can occur during surgery for rectal cancers. Lymphatic and hematogenous spread occurs primarily to the liver.
Patient Simulation & Special Considerations: Rectum & Anus
In treating the rectum and anus, the simulation process is consistent with the typical pelvis (anchor1), with the addition of a few considerations. Depending on the doctor’s preference, an external radiopaque marker may be placed on the anal verge for visualization to ensure adequate coverage of the tumor. Due to the shallow location of the anus, bolus may be necessary to bring the dose more superficial. Prone positioning is easiest for placement of the bolus with minimal air gaps. Some patients may benefit from wet or Vaseline-coated gauze to fill gaps under the bolus – consult with the physician and dosimetrists.
Treatment Volume Localization: Rectum & Anus
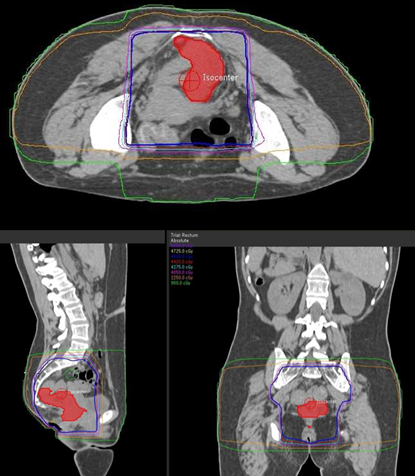
When treating rectal patients, the most common 3D beam arrangement is a 3-field technique: PA field and opposed lateral fields with wedges.
Treatment borders for the rectum and anus are as follows:
- Superior: L5-S1 interspace
- Inferior: 5 cm below the tumor; below obturator foramina
- Lateral: 1-2 cm beyond the pelvic inlet
- Anterior: Anterior to or mid-acetabulum for a standard lateral field; anterior to the pubic symphysis to include the external iliac nodes (if needed)
- Posterior: Posterior to the sacrum

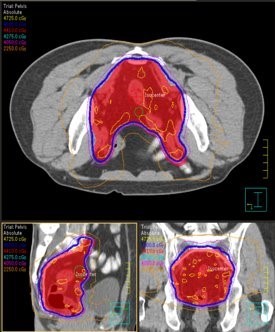
IMRT and VMAT treatments still follow these general borders but are more conformal to targeted tissues, sparing normal tissues, and reducing toxicity. Please refer to the “Treatment Volume Location: Pelvis” section.
Treatment Techniques: Rectum & Anus
Surgery is the treatment of choice for rectal cancer. Radiation therapy is used as an adjuvant treatment, either before or after surgery with chemotherapy. Preoperative radiation therapy reduces the risk of tumor seeding in surgery, shrinks the tumor, and treats the tumor when it has better oxygenation and is therefore more radiosensitive. Postoperative radiotherapy has the advantage of knowing the geographical extent of disease for treatment planning. Patients with residual postoperative disease are referred to radiotherapy.
The dose fractionation for rectal cancer includes:
- Standard Course: 45 Gy in 25 fractions of 1.8 Gy in 5 weeks with a boost of 5.4 Gy in 3 fractions
- Postoperative radiation therapy: 45 Gy in 25 fractions of 1.8 Gy in 5 weeks with a boost of 5.4-9 Gy in 3-5 fractions
- Short Course: 25 Gy in 5 fractions of 5 Gy in 1 week
Adjuvant chemotherapy has the benefit of decreased disease recurrence and improved survival rate. Common chemotherapy drugs that may be given are 5-FU, Cisplatin, and Mitomycin C.
Anal cancer is usually treated by radiation therapy with or without chemotherapy. Radiation therapy consists of delivering 45 to 50 Gy to the entire pelvis, inguinal lymph nodes, and the perineum. A boost of 15 to 20 Gy is then given to the primary tumor. Interstitial implants may also be used.
Treatment techniques that can be used in rectal and anal cancer cases coincide with the techniques used in many other pelvic regions, such as three-field, four-field, IMRT/VMAT, and IORT.
Media Attributions
- Diagram showing the anatomy of the anus CRUK 282 © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- DRRs for a 3-field treatment plan for a cancer of the rectum © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- 3-field treatment plan for a cancer of the rectum © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- IMRT plan for a cancer of the rectum and pelvic nodes © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
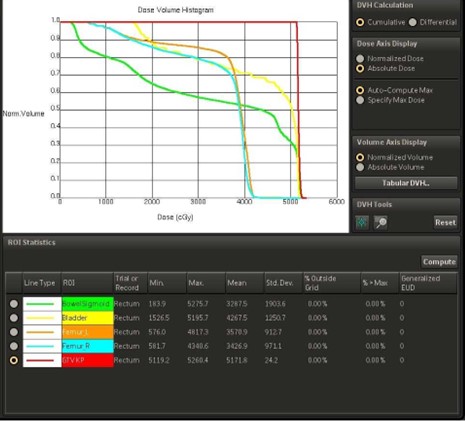
- DVH for a 3-field treatment plan for a cancer of the rectum © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license

{kind=link}