
22 Whole Abdomen Irradiation (WAI)
Whole abdomen irradiation (WAI) is less common today but historically was used in treating cancers that have an increased likelihood to spread to the abdominal cavity referred to as “peritoneal seeding.” Gynecological malignancies, primarily ovarian cancers, and some pediatric cancers like neuroblastoma and Wilm’s tumors benefit from this treatment. Due to the large field size and volume of irradiated tissues, WAI causes acute nausea, fatigue, vomiting, diarrhea, loss of appetite, and myelosuppression. Late toxicities include enteritis, small bowel obstruction, late renal and hepatic injury, and fistula. Today alternative treatments produce similar outcomes with reduced side effects.
Patient simulation & Special Considerations: WAI
The patient setup for a whole abdomen follows the general guidelines described in the Patient Simulation: Abdomen section. If the patient is unable to bring their arms above their head, they can be placed akimbo along the patients side, making sure they’re away from their body as far as possible. Some patients may benefit from using a strap to support their arms.
Treatment Volume Localization: WAI
The beam arrangement for WAI is AP/PA. Due to the kidneys’ low tolerance dose, blocks are used during WAI to decrease the kidneys dose. Anatomically the kidneys are positioned more posteriorly in the body, therefore, divergence will cause the posterior beam blocks to be larger than the anterior blocks. Three methods can be used to shield the kidneys:
- Kidney blocks are added during treatment once their tolerance dose is met. This was generally considered the best option because it ensured that the kidneys received their target dose or as much dose as possible if the patient discontinues treatment before the entire prescription is delivered.
- Blocks that allow partial beam transmission are used for the entire radiation course.
- Kidneys are fully shielded for the AP or PA treatment field for the entirety of the treatment.
Even with kidney blocks, a significant dose (10-15%) will still reach the kidneys due to internal scatter. Transmission of the beam, approximately 3%, is also possible through the blocks and leaves. The dose transmitted through the blocks depends on the size of the irradiated area, beam energy, and block size. Liver blocks can also shield the right lobe of the liver after 25 Gy is delivered.
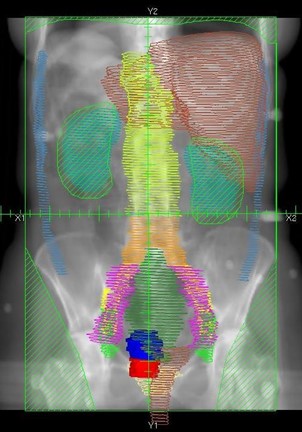
The borders for whole abdomen irradiation are:
- Superior: 1-2 cm above the dome of the diaphragm; the margin is best determined under fluoroscopy, with the patient breathing quietly due to the constant motion of the diaphragm.
- Inferior: Include the entire pelvic floor and to the bottom of the obturator foramen.
- Lateral: Include the peritoneal cavity
Treatment Techniques: WAI
Gynecological treatments using whole abdominal irradiation deliver 1.25-1.5 Gy per fraction to a total dose of 30 Gy. The initial treatment may have a boost to the pelvis and the paraaortic lymph nodes. The boost to the pelvis is delivered with 1.8 Gy per fraction to a total dose of 45-50 Gy. A boost given to the paraaortic and pelvic lymph nodes is treated to a dose of around 42 Gy, depending on the presence of gross disease.
Standard energies for this treatment vary based on patient thickness. Most treatment plans utilize 6 MV photons, but 10 MV is used for thicker patients. This energy consideration is necessary due to the variation in dmax.
Whole-abdominal treatment fields need to minimize the amount of bone marrow, lung, and heart in the radiation field. AP/PA beam arrangements often deliver adequate doses to the whole abdomen but require large treatment fields. A critical organ tolerance dose is the kidneys. For an adult, the dose to the whole kidneys must be limited to 20 Gy; for a child, the dose must be below 15 Gy. The liver is another critical organ with a tolerance dose of 30 Gy. Liver blocks are also added after the delivery of about 25 Gy.
Emerging Technologies & Treatments: WAI
IMRT/VMAT: Technology advancements in treatment planning and delivery are making it possible to deliver treatments to large treatment fields like those required for WAI. If the field is too large for a single field, an important consideration is the “match” between fields where the doses are blended and the longitudinal shift. This treatment technique can help deliver a more uniform dose to the abdomen and reduce the dose to the kidneys.
TomoTherapy offers possibility of irradiating large target volumes continuously and homogeneously without gapes and junctions. This ensures irradiation of entire abdomen in one session, short treatment times, and a full 360-degree treatment. Elective dose reduction to OARs and direct image verification of patient position via CT.
Media Attributions
- Radiation Whole Abdomen1 © Tdvorak is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}