
10 Larynx
The larynx is comprised of the glottis, supraglottis, and subglottis, with the largest of these three regions being the supraglottis. Approximately 65% of cancers occur in the glottis, 34% in the supraglottis, and 1% in the subglottis. Treatments vary depending on the stage and origin of the malignancy.
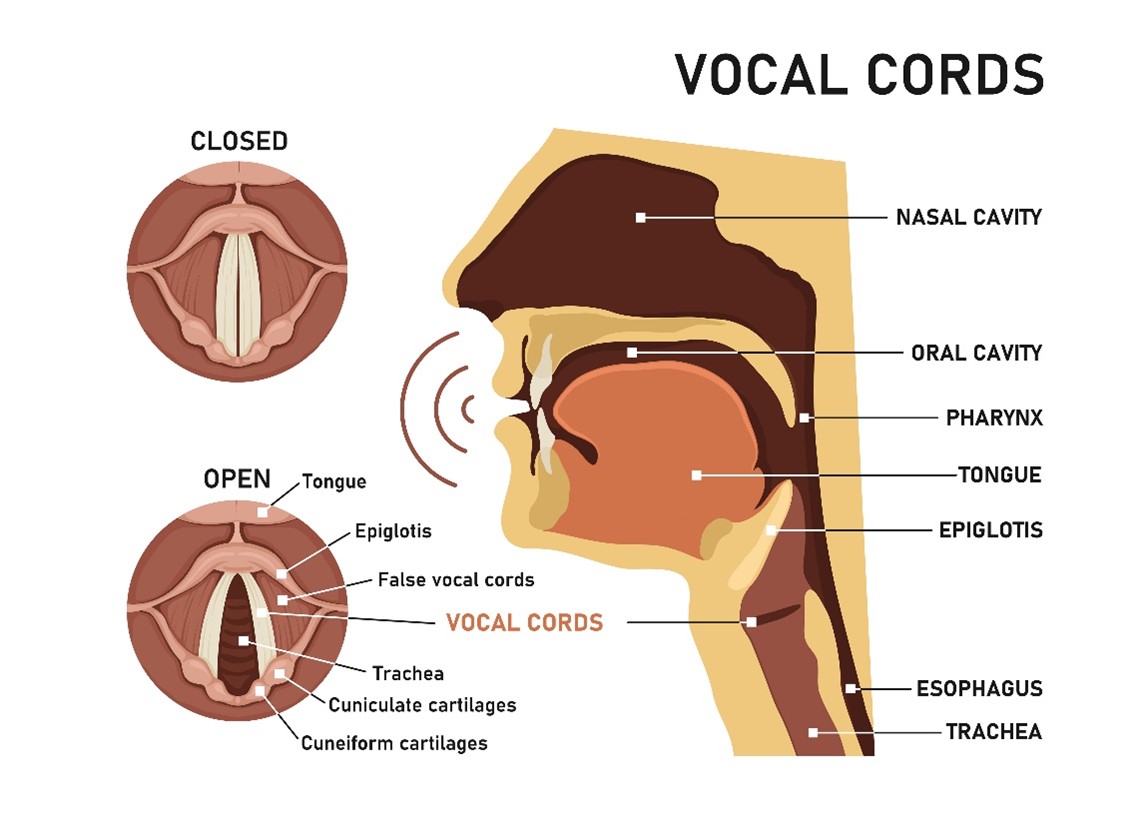
The larynx extends from the epiglottis to the cricoid cartilage at the level of C3 to C6. The supraglottis region includes the epiglottis, false vocal cords, ventricles, aryepiglottic folds, and arytenoids. The glottis region consists of the true vocal cords and the anterior and posterior commissures, and the subglottis region is located 1 cm below the true vocal cords. Cancer of the larynx is strongly associated with cigarette smoking and HPV; most tumors are squamous cell carcinoma (SCC). HPV+ patients have an improved prognosis through the use of targeted therapies.
Simulation Overview & Special Considerations: Larynx
In treating the larynx, the simulation process is consistent with the typical head and neck simulation. Please refer to the “Patient Simulation: H&N” section.
Considerations when simulating patient with cancer of the larynx include using a headrest that extends their chin. The patient’s shoulders should be low to keep them out of the lateral radiation treatment beams. A thermoplastic head and shoulder mask should be made while the patient relaxes their shoulders down or reaches towards their toes until the mask has cooled. Straps can also be used around the patient’s wrists with their knees bent, having the patient straighten their legs on the strap, depressing their shoulders. It is important to document the length and position of the straps for reproducibility.
Shoulder retraction, a Civco device demo.
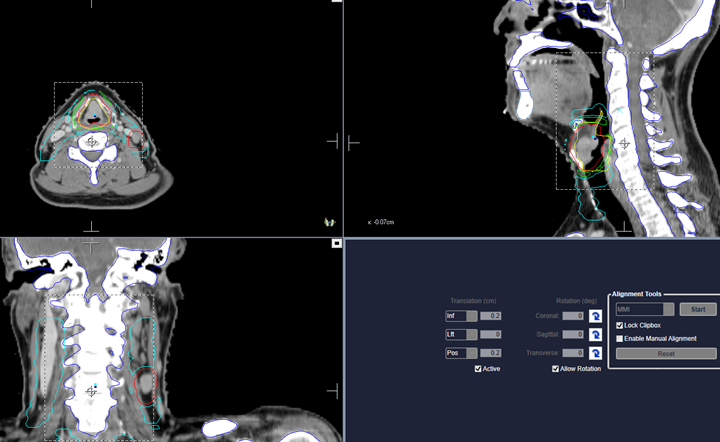
Treatment Volume Localization: Larynx
Supraglottic tumors spread to the jugulodigastric lymph nodes, the superior deep lymph nodes, and the mid-jugular lymph nodes. Treatment borders for the supraglottis and T3/T4 positive lymph node glottic cancers depend on the extent of spread. T3/T4 lesions, the treatment fields should encompass the lower jugular lymph nodes and the supraclavicular lymph nodes. Advanced glottic and supraglottic cancers will follow standard IMRT treatment margins; please refer to the “Treatment Volume Location: H&N” section.
Cancers of the true vocal cords, frequently called glottic cancers, spread through local invasion to the subglottic and supraglottic regions. However, most glottic cancers are detected early, and invasion is rare. Laryngeal tumors can spread lymphatically to Rouviere’s lymph nodes through local extension or direct invasion. Metastasis rarely occurs unless the tumor spreads outside the true vocal cords; metastasis to the lung is the most common.
For treatment fields, the treatment portal for T1 lesions of the glottis is limited to the vocal cords. Lymphatics spread is rare; therefore, they are not included in the treatment ports. Early-stage (T1 & T2) glottic cancer is treated with parallel-opposed lateral fields and wedges.
The treatment borders include:
- Anterior: 1.5-2 cm beyond the thyroid cartilage (flash over skin)
- Posterior: Anterior margin of the vertebral bodies
- Superior: Top of the thyroid cartilage
- Inferior: Below the cricoid cartilage
Advanced T2 lesions are planned to have a 2-3 cm margin around the tumor and the jugulodigastric and mid-jugular lymph nodes are encompassed in the portals.
Advanced T2 Tumors of the glottis Treatment Borders:
- Anterior: 1.5-2 cm beyond the thyroid cartilage
- Posterior: Mid-vertebral bodies
- Superior: Supraglottic extension and 2-3 cm margin
- Inferior: Infraglottic extension and 2-3 cm margin
Treatment Techniques: Larynx
External Beam Radiation Therapy (EBRT) is the preferred treatment technique for early-stage glottic cancer as it helps to preserve voice quality and produce favorable cure rates; it is best when treating early-stage supraglottic lesions with minimal local extension. Broad-shouldered patients may need couch kicks to avoid treating the shoulders. A 15–30-degree wedge is commonly used to achieve a more uniform dose distribution across sloping skin surfaces of the anterior neck.
Advanced lesions of the glottic larynx are typically treated with a total laryngectomy and radical neck dissection, and postoperative radiation can be prescribed “salvage therapy” if needed. Patients with advanced disease and protocol patients can undergo concurrent radiation therapy and chemotherapy, whereas patients with fixed vocal cords should only receive radiation therapy. For patients with inoperable disease, radiation therapy can be prescribed for palliation.
| Location / Stage of Disease | Beam Orientation & Dose | Sites included |
| Early-Stage Glottis (T1 & T2) | Opposed laterals; 4-6 MV; 60-66 Gy | Larynx |
| T3 & T4 Glottis | IMRT/VMAT; 4-6 MV; 70 Gy | Primary tumor and regional lymphatics |
| Glottic w. extension to Supraglottis or Subglottis | IMRT/VMAT; 4-6 MV; 74 Gy | Primary tumor and regional lymphatics |
Regional lymphatics include the supraclavicular and lower jugular lymph nodes. All treatments curative treatments have a goal of minimal functional impairment. Modern IMRT margins are reflected in the “Treatment Techniques: H&N” section for advanced cancers of the larynx and supraglottis.
Media Attributions
- Picture18 © Adobe stock: 310857942
- Picture19 © The University of Iowa Radiation Therapy Program
