
21 Kidney, Wilms, & Neuroblastoma
Overview: Kidney, Wilms, & Neuroblastoma
The kidneys are retroperitoneal structures located between the T12 and L3 vertebrae. The right kidney is commonly situated more inferior than the left due to the position of the liver. Renal lymphatics consist of the paraaortic and lumbar nodes. Primary tumors of the kidney in adults are commonly renal cell pathology. Wilms tumors, also known as nephroblastoma, are the most common type of pediatric kidney cancer. They are classified as either favorable histology or anaplastic histology.
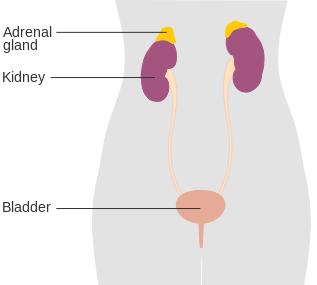
The adrenal glands sit on top of each kidney. They produce hormones that regulate the body’s immune system, blood pressure, metabolism, response to stress, and other essential functions. Adult malignancies of the adrenal glands are commonly metastatic. However, primary pediatric tumors of the adrenal glands are termed neuroblastoma. These tumors are the most common extra-cranial malignancy found in children and are the most common malignancy before age 1. They originate from early forms of sympathetic nerve cells termed Primitive Neuroectodermal Tissues (PNET), most often found in an embryo or fetus. PNET-associated tumors can occur anywhere in the body, but are most commonly found in the adrenals.
|
Malignancy
|
Wilms Tumor
|
Neuroblastoma
|
|
Age
|
Older (3-4 years)
|
Less than 18 months
|
|
Systemic Symptoms
|
No
|
Yes
|
|
Calcifications
|
No
|
Yes
|
|
Location
|
Kidney
|
Adrenal gland
|
|
Crosses midline
|
Not typical
|
May cross
|
|
Fixed/immobile
|
May be displaced
|
Fixed/immobile
|
Patient Simulation & Special Considerations: Kidney, Wilms, & Neuroblastoma
The simulation procedure for cancers of the kidneys and adrenal glands follow the general guidelines found in the Patient Simulation: Abdomen section. However, special consideration should be given to the use of intravenous contrast. Kidney function is reduced and these using iodinated contrast may be contraindicated – be sure to consult with the physician and review recent kidney function lab results. Additionally, the amount of contrast needed for pediatrics is based on the patient’s weight if it’s used, it’s important to follow the institution’s protocol. Pediatric patients may also need anesthesia to complete the simulation process and daily treatment – coordination of care is important. Treatment first thing in the morning is best for npo requirements.
Treatment Volume Localization: Kidney, Wilms, & Neuroblastoma
Surgery, if possible, and chemotherapy are the primary treatment options for cancers of the kidneys and adrenal glands. Radiation therapy is recommended for advanced and aggressive disease or for palliation to relieve symptoms such as pain, bleeding, or other problems caused by cancer spread. The Organs at Risk (OARs) to consider are the small bowel, liver, spinal cord, and unaffected kidney. The remaining kidney should receive no more than 1800 cGy for functional preservation purposes. It is important to spare as much of the liver as possible, especially if treating on the patient’s right side. For specific TD 5/5’s, refer to the Treatment Volume Localization: Abdomen section.
Kidney: Treatment fields consist of the post-operative renal bed and paraaortic lymph nodes. Traditionally, treatments included the entire length of the involved ureter. Modern treatment techniques apply a 3-5 mm margin to the PTV. Respiratory management can reduce these margins further.
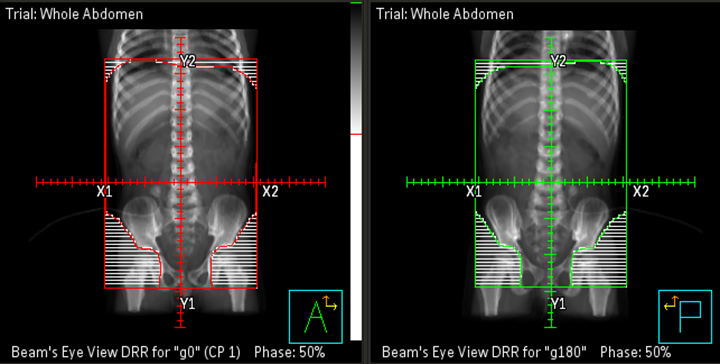
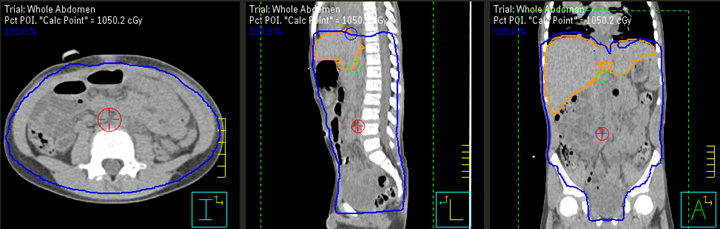
Wilms tumors and Neuroblastoma: Treatment margins are generally determined MRI or CT images and the operative report. Both tumors can grow very large before diagnosis requiring very large treatment fields. Additionally, the entire width of the vertebral bodies should be included to uniformly affect the epiphyseal growth plates on both sides of the spinal column and reduce the incidence of subsequent scoliosis. If the peritoneal cavity tests positive for disease or if the tumor ruptures during surgery, whole abdomen radiation therapy may be recommended.
Preoperative Treatment Field Borders:
- Lateral: Encompass the abdominal wall (outside peritoneal line).
- Medial: Includes the entire width of the vertebral bodies with enough contralateral extension to include the paraaortic lymph nodes while excluding the opposite kidney.
- Superior: Includes the kidney tumor with a 1 cm margin – the field should extend to the dome of the diaphragm only if the tumor goes that high.
- Inferior: Kidney and entire preoperative tumor extent with a 1 cm margin.
IMRT and VMAT treatment treatment options still follow these general borders but are more conformal to targeted tissues, sparing normal tissues, and reducing toxicity. The PTV typically has an expansion of 5 mm depending on the department protocol, equipment availability, and patient’s disease. It is important to continue to consider the potential growth impairment. Treatment fields may require treatment volumes to extend across the midline to preserve symmetry, and care must be taken since some organs may be displaced following surgery. Generally, beam sizes are at least 6 cm.
Treatment Techniques: Kidney, Wilms, & Neuroblastoma
Kidney: The treatment of choice for patients with localized renal cell carcinoma (RCC) T1 and T2 is a radical nephrectomy. This surgery completely removes the intact Gerota’s fascia and its contents. Lymphadenectomy is usually performed as well. Preoperative radiation therapy can shrink the tumor and increase resectability. Postoperative radiation is commonly done to sterilize microscopic disease leftover after surgery. The kidneys are commonly treated with isocentric AP/PA fields. The treatment plans should include equal weighting, bias loading, and other wedge pair techniques.
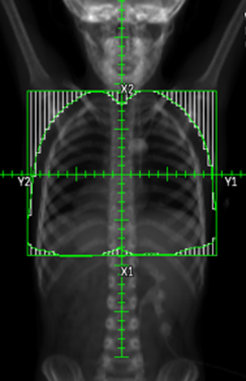
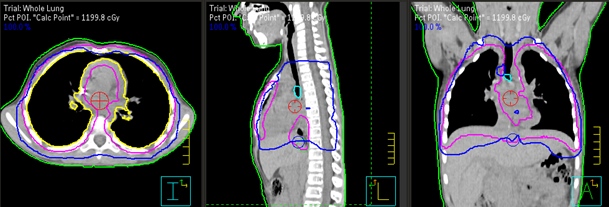
Wilms: Removing the malignant kidney via nephrectomy is the first step in treatment. Regional lymph nodes are biopsied during surgery, and the contralateral kidney is examined for disease. Postoperative radiation therapy of the tumor bed is sometimes given depending on the stage and histologic subtype of the disease. Only when Wilms’s tumor has metastasized to the lungs will whole lung irradiation be employed.
Neuroblastoma: Surgical excision is often the treatment of choice for children with abdominal primary, node-negative disease. Multimodality treatment include:
- Initial chemotherapy followed by surgery. For high-dose chemotherapy, a transplant to replace the bone marrow stem cells damaged by the chemo may need to be performed.
- Retinoid Therapy uses retinoids, which are chemicals related to vitamin A, that help some cancer cells mature into normal cells.
-
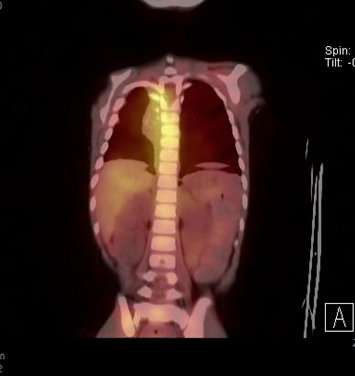
MIBG scan for neuroblastoma. MIBG Radiotherapy uses MIBG, a chemical similar to norepinephrine made by sympathetic nerve cells. A slightly radioactive form of MIBG is sometimes injected into the blood as part of an imaging test to look for neuroblastoma cells in the body. However, a more radioactive form of MIBG can also be used to treat some children with advanced neuroblastoma, often along with other treatments.
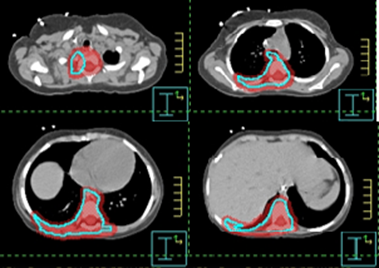
- Radiation Therapy – The dose for neuroblastoma varies depending on the tumor stage, size of fields, and age of the child. For patients with gross residual tumors remaining after surgery and patients with positive lymph nodes, postoperative radiation therapy of the tumor bed with wide margins is beneficial if chemo does not produce a complete response. External beam radiation therapy (EBRT) is used to shrink tumors, which makes them easier to remove. Radiation might be given to the primary tumor area and other areas of the body that might have active disease seen on the MIBG scan.
|
Treatment
|
Doses/Fractionation**
|
|
Kidney: Postoperative
|
|
|
Kidney: Right-sided tumor
|
|
|
Wilms
|
|
|
Neuroblastoma
|
|
Three-dimensional conformal radiation therapy (3D-CRT): With virtual simulation or 3D definition of the GTV, AP/PA beam arrangements with MLC shaping are often still appropriate to produce symmetrical irradiation of the vertebrae, avoid the contralateral kidney and minimize whole body doses.
IMRT/VMAT: Because of multiple constraints and the proximity of vital organs, inverse planning and the use of IMRT may be necessary to achieve an optimal plan for treatment. Delivers a higher dose to the tumor while sparing normal tissue.
Emerging Technologies & Treatments: Kidney, Wilms, & Neuroblastoma
Proton therapy: Ideal for pediatric patients because it offers fewer long-term side effects.
Other treatment advances and technologies available for cancers of the kidneys and adrenal glands are the same as those described in the Emerging Technologies & Treatments: Abdomen section.
Media Attributions
- Diagram showing the position of the adrenal glands CRUK 343 © Cancer Research UK is licensed under a CC BY-SA (Attribution ShareAlike) license
- Whole abdomen DRRs for Wilms tumor © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- Whole abdomen treatment plan for Wilms tumor © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- Whole lung DRR for Wilms tumor © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- Whole lung treatment plan for Wilms tumor © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- MIBG scan for neuroblastoma © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
- Treatment plan based off MIBG scan for neuroblastoma © The University of Iowa Radiation Therapy Program is licensed under a CC BY (Attribution) license
outside the cranium

{kind=link}